Advocates Were Right to Sound the Alarm: Congress Cut Over $1 Trillion from Health Care — And States Are Already Paying the Price
05.21.2026
When Congress debated and ultimately passed H.R. 1 last year, health advocates warned the results would be deadly. Cutting $1 trillion from the health care system — with the majority of it coming from Medicaid — would leave states with no good options: cut coverage, cut benefits, or cut provider payments that millions of low-income Americans depend on. Now, as states finalize their Fiscal Year 2027 budgets, the evidence is rolling in. Unfortunately, advocates were right, and the consequences are landing hard on patients and families.
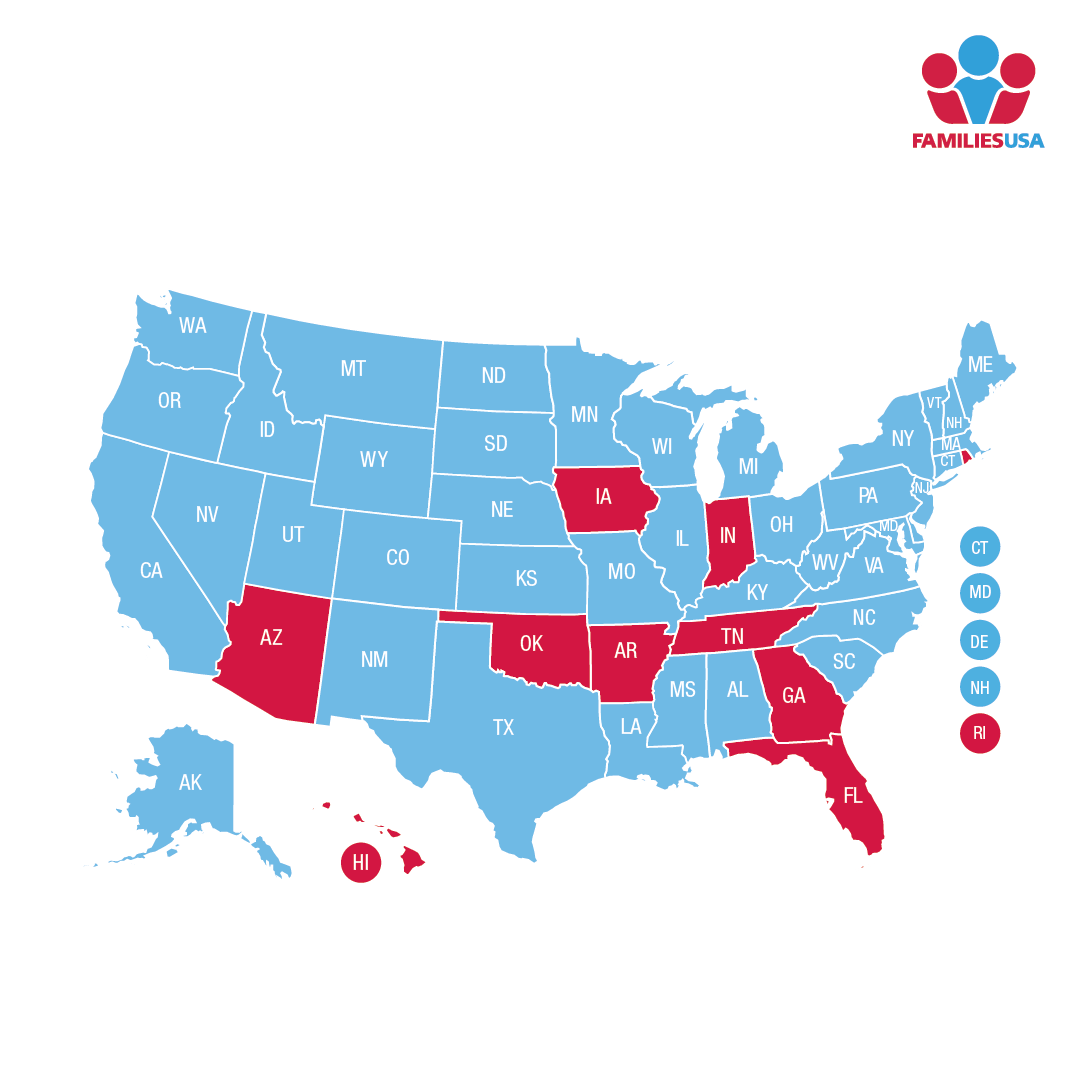
The most drastic cuts included in H.R. 1 don’t go into full effect until January 1, 2027, but states must start preparing to absorb the fiscal shock much sooner. Families USA is tracking state budget decisions across the country to identify ways in which states are responding. Only 20 states have finalized their budgets so far, with many more still in progress. But already the pattern is unmistakable: less money for patient care, more administrative burden for the people who need coverage most.
States Are Cutting Coverage, Care, and Critical Services
For states already running budget shortfalls, there are few options to mitigate the blow of such a massive reduction in federal financial support. Whether a state is directly cutting health care costs or shifting funds away from other important economic support for families, the impact will be immense:
- Cuts to provider rates mean fewer providers willing to accept Medicaid patients.
- Cuts to benefits means people going without the care they need.
- Less funding available for other state economic support programs means families may have to make more sacrifices that impact their health — like skipping meals or not turning on their air conditioning.
These are the direct, predictable consequences of what Republican lawmakers and President Trump chose to do — and this is just the first year of a decade of cuts to come.
The early budget data confirms several states are making sweeping overall cuts to their Medicaid programs:
- Colorado was forced to pass a budget with $135 million in cuts to provider rates and Medicaid services.
- Florida lawmakers are currently negotiating with their governor over budget proposals that will cut $206 million from Medicaid managed care plans on top of other proposals to cut more than $89 million for hospital services.
- Idaho lawmakers voted to proceed with a three percent across-the-board cut to Medicaid, meaning fewer services for everyone enrolled.
- Kentucky took particularly harsh measures, choosing to allocate $691 million less to Medicaid over two years than its own state agency said it needed – a deliberate shortfall that will be felt by patients, not politicians.
Several states are explicitly proposing or enacting budgets that cut enrollment or benefits in their budgets:
- Arizona lawmakers are proposing eligibility and enrollment restrictions that are more stringent than H.R. 1, like quarterly eligibility checks, as part of a package that would generate $180 million in budget cuts across multiple programs.
- California is considering bringing back asset test limits in Medicaid for seniors who have more than $2,000 in cash or other financial resources, which is expected to result in 25,000 seniors losing eligibility in FY2026-27 and 62,000 seniors losing eligibility in FY2027-28.
- Colorado will extend its waitlist for 24/7 care for adults with developmental disabilities by only enrolling one new member for every two spots vacated. This change is expected to double the waiting period for services from 7 to 14 years.
Other states are covering Medicaid budget shortfalls by shifting hundreds of millions of dollars away from other state funds that would otherwise support other essential services such as housing, food assistance, or child care:
- California is considering filling its Medicaid budget hole caused by H.R. 1 in FY2026-27 with $1.5 billion in new general fund spending.
- Iowa is addressing pre-existing Medicaid budget shortfalls of $90 million in FY2026 and $167 million in FY2027, in addition to new shortfalls created by H.R. 1, by temporarily increasing a managed care plan tax, and shifting $89 million in general fund dollars and $350 million from Iowa’s Taxpayer Relief Fund to its Medicaid budget.
- Michigan is proposing to cover H.R.1 federal spending reductions and implementation costs by shifting $186 million from the state’s general fund.
The Hidden Cost: States Are Spending Real Dollars to Implement Congressional Red Tape
Here’s the part that rarely makes headlines but deserves attention: H.R. 1 doesn’t just cut Medicaid funding — it mandates a sweeping set of new administrative requirements that cost states real money to implement. Work reporting requirements, more frequent eligibility redeterminations, immigration status verifications, and new enrollment restrictions all require states to build new or upgraded eligibility and enrollment systems from scratch.
CMS is providing $200 million in one-time federal funds to help — but that falls far short of what states actually need to build the comprehensive eligibility and enrollment system infrastructure that is required. As a result, the gap must be filled with state dollars. For example, Kentucky has budgeted $9.6 million just for the technology to implement H.R. 1 work reporting requirements. Utah has funded $16.5 million for H.R. 1 Medicaid eligibility implementation. Colorado has budgeted $19.1 million to upgrade its eligibility systems. And Arizona estimates that it will need $65 million for implementation.
Of course, investing in Medicaid data infrastructure and eligibility systems can be genuinely valuable — for care management, fraud detection, and making sure the right people get the right benefits. This is not that. These systems are being built to implement congressional mandates whose primary effect is to make it harder for eligible people to enroll and stay enrolled. States are spending tens of millions of dollars not to improve care, but to implement a massive disenrollment system.
Congress made a deliberate choice to cut health care coverage for millions of Americans to help pay for tax cuts for the wealthy. Health advocates, clinicians, and state officials warned exactly what would happen. The 2026 state budget season is the first chapter of that story being written in real numbers, causing real harm to real people.
Families USA will keep tracking every state budget as it is finalized. As the full picture comes into focus, one thing is already clear: the cost of H.R. 1 is not being borne by the special interests that lobbied for it. It is being borne by the patients, providers, and states whose clear warnings went ignored by politicians who chose not to stand up for the communities they were elected to represent.
related content